Spondylolysis
Description:
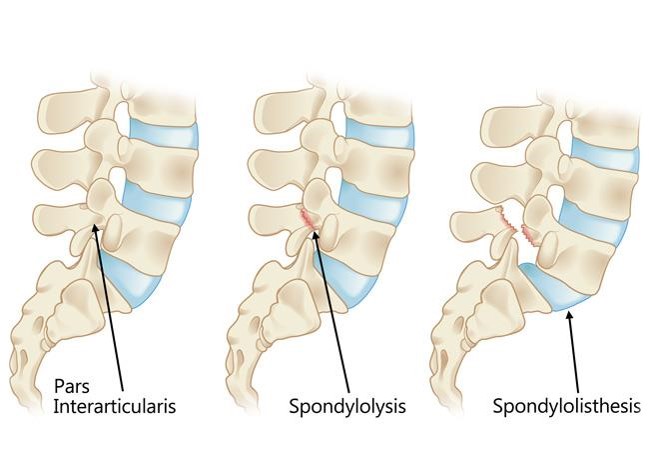
Spondylolysis is a unilateral or bilateral bony defect in the pars interarticularis or isthmus of the vertebra. The term derives from the Greek words spondylos (vertebra) and lysis (defect). It can cause a slipping of the vertebra.
Relevant anatomy:
Vertebrae consist of the vertebral body and a bony ring or arcus which protects the spinal cord.The arcus is formed by two pedicles which attach to the dorsal side of the vertebral body and two laminae, which complete the arch.
The area between the pedicle and the lamina is called the pars interarticularis and is in fact the weakest part of the arcus. It is the pars interarticularis that is affected in spondylolysis.

Aetiology:
Affects 3-6% of population. This condition appears in the first or
second decade of life; the frequency of spondylolysis increases with age until
20 years.
Men are affected twice as often as women. There is a possible genetic tendency for people with lower cortical bone density at the pars interarticularis. Spondylolysis occurs more frequently in the young athletic population. There is an increased risk in gymnasts, football players, cricketers, swimmers, divers, weight lifters and wrestlers.
Spondylolysis is considered to be a stress fracture that results from mechanical stress at the pars interarticularis. These stress fractures occur due to repetitive load and stress, rather than being caused by a single traumatic event.
The stress distribution at the pars interarticularis is the highest in extension and rotation movements. Spondylolysis occurs mostly at L5 (80-95%) due to repetitive hyperextension, which increases the contact between the caudal edge of the inferior articular facet of L4 and the pars interarticularis of L5.

Clinical presentation:
in most cases, spondylolysis is asymptomatic. If there are an symptoms, they often have following characteristics:
• Onset of pain is gradual or acute (after intense athletic activity)
• Possible history of local trauma (recent or historical)
• Intense pain restricts activities of daily living or sporting performance
• Symptoms become aggravated after a stressful event
• Rest usually relieves the symptoms
Specific symptoms depend on the region of the spine that is affected. Lumbar spondylolysis will show different symptoms than thoracic or cervical spondylolysis. Symptoms for lumbar spondylolysis are as followed:
• Focal low back pain with radiation into the buttock or proximal lower limb
• Symptoms can increase with movement specifically lumbar extension or rotation
• Children under 13 years old show tenderness or pain on extension
• Children can present a postural deformity or abnormal gait pattern
• Pain throughout lumbar range of movement
Differential diagnosis:
• Disc Injuries: Disc Herniation
• Acute Bony Injuries
• Sprain/Strain Injuries
• Spondylolisthesis
• Myofascial Pain in Athletes
• Sacroiliac Joint Injury
• Lumbar radiculopathy
• Osteomyelitis
• Spinal stenosis
Procedure of diagnosis:
The golden standard for the diagnosis of spondylolysis is the combination of SPECT and computed tomography (CT). When a pars fracture is present, computed tomography can clearly visualize the spondylolysis.
On axial CT scans, the neural arch should be closed and continuous at the level of the pedicles. When there is a pars defect, there is a discontinuity at this level. Sagittal CT images differentiate better between a pars defect and the facet joint and are also the most accurate in showing incomplete fractures.
MRI shows promising results in detecting spondylolysis but can also be used to determine the state of the disc above and below the affected vertebra.
Examination:
The most common findings for lumbar spondylolysis are hyperlordotic posture and low back pain during lumbar extension.
The Michelis' test or unilateral extension test can be performed to confirm diagnosis. The patient performs hyperextension of the lumbar spine while standing on one leg. In a positive test, pain is reproduced. Unilateral lesions often produce pain when standing on the ipsilateral leg.
Neurologic exam is usually normal but neurogenic symptoms can arise if the condition progresses to spondylolisthesis
Medical management:
Conservative treatment is usually sufficient to treat symptomatic spondylolysis and aims to reduce pain and facilitate healing processes.Possible conservative treatments are:
• NSAIDs for pain relief
• cessation of aggravating (sporting) activities
• the use of a spinal brace to prevent motion at the injured pars and allow bony repair
• Physical therapy
When severe pain is persistent, progression to spondylolisthesis needs to be prevented: surgical treatment may be required. This only occurs in some patients and evidence of long-term benefit is still uncertain.
Latest procedures attempt a repair of the affected pars with preservation of the segmental mobility whereas earlier methods sometimes included a spinal fusion procedure.
Physiotherapy management:
• Facilitating the healing processes by promoting additional blood flow and thus healing of the affected pars. This can be accomplished by isometric contractions of the surrounding muscles.
• Avoiding aggravation or turning into a chronic state by handling underlying causes (e.g. hypermobility, hyperextension in specific sports such as wrestling or skating)
• Optimization of physical function
• Global and specific strengthening exercises
• Reduce pain
• Promoting normal movement patterns
Rehabilitation programme should progress in 4 stages:
• Control pain and inflammation: Taking stress off the injured area allows physiological healing processes to take place.
• Therefore, it may be necessary to avoid rotational shearing forces and extension movements by a temporary cessation of sporting activities and/or wearing a brace.
• It reduces the pain intensity and functional disability levels.
• Strength and flexibility: As paraspinal muscle spasms and hamstrings tightness are often seen in patients with spondylolysis, stretching exercises can be added to the rehabilitation program. Flexibility training is useful in patients with hypomobility of the spine.
• A global strengthening program should be started which can include specific back strengthening exercises.
• Stabilization: Neuromuscular stabilization techniques, including activation of transversus abdominis and other core stabilizer muscles have be shown to decrease pain in some older research. This section includes education and postural training. There is evidence suggesting that specific trunk stabilizing exercises to spondylolysis.
• Functional movement: The main goal of physiotherapy is to increase functional abilities through a home exercise program. As soon as primary pain decreases, patients have to be encouraged to resume activities as tolerated.
A detailed knowledge of spinal anatomy and maintaining patient function/quality of life is imperative. Objective interpretation of medical imaging is necessary in order to avoid making premature conclusions because there is a low correlation between clinical findings and symptoms. Due to the athletic background of most patients with spondylolysis, it is essential to be well informed about training principles and sports-specific exercises to provide the patient with the best care available.


Comments
Post a Comment